MALIGNANT BRAIN TUMOR
Glioblastoma (GBM), also referred to as a grade IV astrocytoma, is a fast-growing and aggressive brain tumour. It invades the nearby brain tissue, but generally does not spread to distant organs. GBM is a devastating brain cancer that can result in death in six months or less, if untreated.
The mainstay of treatment for GBMs is surgery, followed by radiation and chemotherapy. The primary objective of surgery is to remove as much of the tumour as possible without injuring the surrounding normal brain tissue needed for normal neurological function. However, GBMs are surrounded by a zone of migrating, infiltrating tumour cells that invade surrounding tissues, making it impossible to ever remove the tumour entirely. Surgery provides the ability to reduce the amount of solid tumour tissue within the brain, remove those cells in the centre of the tumour that may be resistant to radiation and/or chemotherapy and reduce intracranial pressure. Surgery, by providing a debulking of the tumour, carries the ability to prolong the lives of some patients and improve the quality of remaining life.
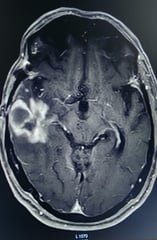


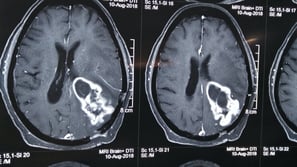
Tumour in left dominant temporal brain.
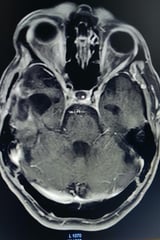
Subtotal removal of tumour


Eloquent cortex is a term that refers to specific brain areas and its associated subcortical structures that directly controls function, thus damage to these areas generally produces major focal neurological deficits. Unlike cancers affecting other solid organs, brain tumours grow within the context of complex neural circuitry. Regardless of location, all intrinsic brain tumours interface with nervous system structures.
Many intrinsic brain tumours arise within eloquent cortical and subcortical regions of the brain. It is therefore critical that surgery for tumour removal balances both the oncological benefits of maximal resection with preservation of functional neural networks. This goal is achieved with various technological advances like MRI, intra-operative Navigation or ultrasound, cortical mapping and awake anaesthesia, to name a few.
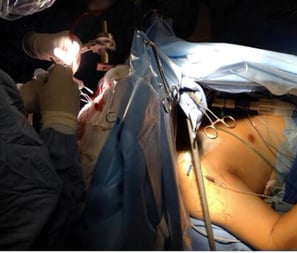
The surgery for such tumours require transdisciplinary work of the Neurosurgeon, Neuroanaesthesiologist and Neuropsychologist before, during and after the resection of a neoplasm in eloquent areas with the patient conscious under the 3A anaesthesia modality (asleep, awake, asleep). This help is taken from other modalities like neuro navigation or intra-operative mapping of motor strip.
Benefits of awake craniotomy are greater resection of the lesion, with improvement in survival, while the damage to the eloquent cortex, which generates postoperative neurological dysfunction, is minimized. Other advantages include shorter hospitalization times, hence a reduction in care costs, and a decrease in the incidence of postoperative complications.
1. ELOQUENT AREA TUMOUR

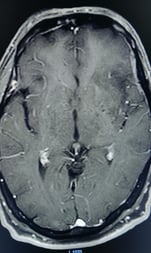
Intrinsic brain tumour in speech area.
Here the patient is awake, whilst the brain surgery is being done.
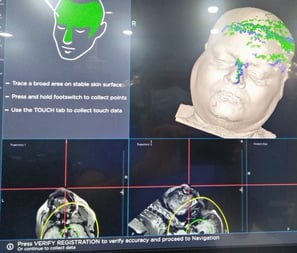
Neuro-navigation during surgery
Motor strip glioma resected with cortical mapping and navigation control
Intra-operative cortical stimulation






2. INSULAR GLIOMA IN DOMINANT HEMISPHERE
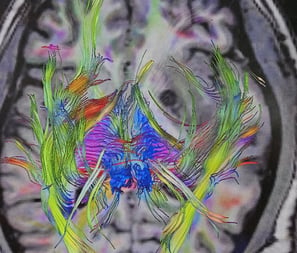
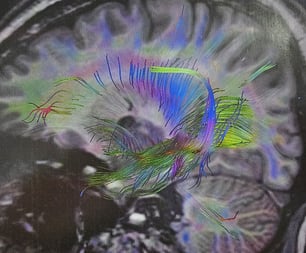
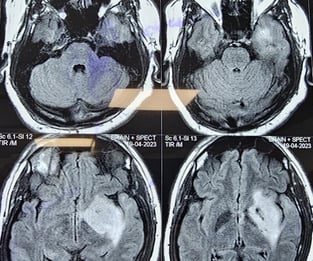
Insular gliomas are complex malignant tumor located in deeper part of brain. This tumor are difficult to operate because they are hidden by the normal brain structures and they are draped over by important blood vessels supplying the brain. Most of these tumors are low-grade malignancies and can be treated by surgery with near total removal of tumor. Functional areas of the brain require detailed mapping by Functional MRI (fMRI) AND NEUROPSYCHOLOGICAL TESTING in addition to regular MRI. Sometimes, such surgeries are done under awake anesthesia
Functional MRI
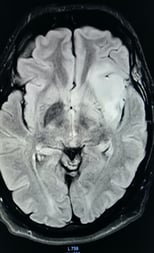
Insular glioma



© Copyright2024 - Dr Ashok Hande - All rights reserved
Clinic Details
Timings: 11 AM - 8 PM
Fortis Hospital
Contact Details for Emergency(24 Hrs)